Pneumocystis carinii:

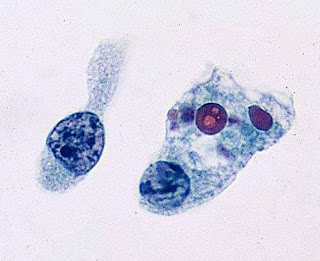
Alveolar cast stained with methenamine silver, showing the typical appearance of the cyst form of the organism. Bronchial washing (methenamine silver × OI).
Pneumocystis carinii Pneumonia:
Before 1960, the organism P. carinii was little more than an academic curiosity. It was rarely diagnosed clinically and, when seen at autopsy, was found to be present almost exclusively in
debilitated premature infants. Pneumocystis carinii pneumonia has been increasing in incidence, however, and is now recognized
as potentially occurring in any situation of impaired immune response. More particularly, it is observed in infants who are premature or debilitated, in patients who have immunologic
disorders and immunoglobulin defects, and in those undergoing therapy with corticosteroids and chemotherapy.
The infection has been found with high frequency in patients who have received renal allografts. The infection has also been
described as a complication in AIDS.The introduction of effective therapeutic drugs has markedly increased the clinical importance of a diagnosis.
Cytology:
On Papanicolaou-stained material, the organisms may be difficult to identify, because their staining may be quite variable and faint. A most typical presentation on the smear is a mass of partially eosinophilic amorphous material. Within this mass may be a suggestion of small superimposed circlets. Although
this presentation may or may not be diagnostic for Pneumocystis, such material should raise an immediate suspicion of its presence,
and the material should be further evaluated by special stains. In such a situation, one would decolorize this slide and restain with methenamine silver. This procedure immediately brings out the diagnostic features of these organisms. On methenamine silver stains, the organism is seen mainly as a spheric cyst measuring 6–8 μm in diameter, or approximately the diameter of an erythrocyte. Certain variations of this form can be seen: The organism can be cup shaped, crescent shaped,
or crinkled. Depending on which surface of the organism is exposed to view, small interior structures can be seen to take the forms of rings, dots, or commas. Some laboratories prefer to use a Giemsa stain or toluidine blue for identification of this organism. With these stains, one is able to identify as many as
eight trophozoites occurring within the cyst. These structures are about 0.5–1.0 μm in diameter. They are easily overlooked and
may be confused with granules or cell fragments.(Ref:Comprehensive Cytopathology,Bibbo)
If you like, you can visit our youtube channel and facebook page👇🏻
Youtube channel link-https://m.youtube.com/channel/UCPGvHc5Ttw4EtB72WVMiYSw/videos
Facebook page link-https://m.facebook.com/PathologyDiscussionForum/?ref=bookmarks

Alveolar cast stained with methenamine silver, showing the typical appearance of the cyst form of the organism. Bronchial washing (methenamine silver × OI).
Pneumocystis carinii Pneumonia:
Before 1960, the organism P. carinii was little more than an academic curiosity. It was rarely diagnosed clinically and, when seen at autopsy, was found to be present almost exclusively in
debilitated premature infants. Pneumocystis carinii pneumonia has been increasing in incidence, however, and is now recognized
as potentially occurring in any situation of impaired immune response. More particularly, it is observed in infants who are premature or debilitated, in patients who have immunologic
disorders and immunoglobulin defects, and in those undergoing therapy with corticosteroids and chemotherapy.
The infection has been found with high frequency in patients who have received renal allografts. The infection has also been
described as a complication in AIDS.The introduction of effective therapeutic drugs has markedly increased the clinical importance of a diagnosis.
Cytology:
On Papanicolaou-stained material, the organisms may be difficult to identify, because their staining may be quite variable and faint. A most typical presentation on the smear is a mass of partially eosinophilic amorphous material. Within this mass may be a suggestion of small superimposed circlets. Although
this presentation may or may not be diagnostic for Pneumocystis, such material should raise an immediate suspicion of its presence,
and the material should be further evaluated by special stains. In such a situation, one would decolorize this slide and restain with methenamine silver. This procedure immediately brings out the diagnostic features of these organisms. On methenamine silver stains, the organism is seen mainly as a spheric cyst measuring 6–8 μm in diameter, or approximately the diameter of an erythrocyte. Certain variations of this form can be seen: The organism can be cup shaped, crescent shaped,
or crinkled. Depending on which surface of the organism is exposed to view, small interior structures can be seen to take the forms of rings, dots, or commas. Some laboratories prefer to use a Giemsa stain or toluidine blue for identification of this organism. With these stains, one is able to identify as many as
eight trophozoites occurring within the cyst. These structures are about 0.5–1.0 μm in diameter. They are easily overlooked and
may be confused with granules or cell fragments.(Ref:Comprehensive Cytopathology,Bibbo)
If you like, you can visit our youtube channel and facebook page👇🏻
Youtube channel link-https://m.youtube.com/channel/UCPGvHc5Ttw4EtB72WVMiYSw/videos
Facebook page link-https://m.facebook.com/PathologyDiscussionForum/?ref=bookmarks
Follow our facebook page for recent articles/videos

Comments
Post a Comment
Thank you for posting your comment.Your question will be answered soon.